
 ,
Ee Teng Goh,
Benjamin Tan,
Abhiram Kanneganti,
Melanie Almonte,
Alasdair Scott,
Guy Martin,
Jonathan Clarke,
Viknesh Sounderajah,
Jan Przybylowicz,
,
Ee Teng Goh,
Benjamin Tan,
Abhiram Kanneganti,
Melanie Almonte,
Alasdair Scott,
Guy Martin,
Jonathan Clarke,
Viknesh Sounderajah,
Jan Przybylowicz,
Competing Interests: JK has received an educational grant from Johnson and Johnson. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
The Covid-19 pandemic has placed unprecedented pressure on healthcare systems and workers around the world. Such pressures may impact on working conditions, psychological wellbeing and perception of safety. In spite of this, no study has assessed the relationship between safety attitudes and psychological outcomes. Moreover, only limited studies have examined the relationship between personal characteristics and psychological outcomes during Covid-19. From 22nd March 2020 to 18th June 2020, healthcare workers from the United Kingdom, Poland, and Singapore were invited to participate using a self-administered questionnaire comprising the Safety Attitudes Questionnaire (SAQ), Oldenburg Burnout Inventory (OLBI) and Hospital Anxiety and Depression Scale (HADS) to evaluate safety culture, burnout and anxiety/depression. Multivariate logistic regression was used to determine predictors of burnout, anxiety and depression. Of 3,537 healthcare workers who participated in the study, 2,364 (67%) screened positive for burnout, 701 (20%) for anxiety, and 389 (11%) for depression. Significant predictors of burnout included patient-facing roles: doctor (OR 2.10; 95% CI 1.49–2.95), nurse (OR 1.38; 95% CI 1.04–1.84), and ‘other clinical’ (OR 2.02; 95% CI 1.45–2.82); being redeployed (OR 1.27; 95% CI 1.02–1.58), bottom quartile SAQ score (OR 2.43; 95% CI 1.98–2.99), anxiety (OR 4.87; 95% CI 3.92–6.06) and depression (OR 4.06; 95% CI 3.04–5.42). Significant factors inversely correlated with burnout included being tested for SARS-CoV-2 (OR 0.64; 95% CI 0.51–0.82) and top quartile SAQ score (OR 0.30; 95% CI 0.22–0.40). Significant factors associated with anxiety and depression, included burnout, gender, safety attitudes and job role. Our findings demonstrate a significant burden of burnout, anxiety, and depression amongst healthcare workers. A strong association was seen between SARS-CoV-2 testing, safety attitudes, gender, job role, redeployment and psychological state. These findings highlight the importance of targeted support services for at risk groups and proactive SARS-CoV-2 testing of healthcare workers.
The Covid-19 pandemic has led to an unprecedented strain on healthcare services globally. Considerable changes in healthcare delivery have necessarily taken place. These have included cessation of routine services, repurposing of clinical areas, redeployment of staff to unfamiliar clinical environments [1,2], and in some circumstances, the rationing of services [3]. The impact of these modified working conditions on safety culture and psychological well-being are poorly understood.
Traumatic events or adverse conditions during natural disasters, conflict, and pandemics may lead to burnout [4–6]. Burnout is defined as “a syndrome of exhaustion, depersonalization, and reduced professional efficacy” [7] and leads to poorer patient safety outcomes [8–10]. Burnout is composed of two elements: “exhaustion”, linked to excessive job demands; and “disengagement”, linked to insufficient job resources [11]. During the Covid-19 pandemic healthcare systems have faced rising demands and limited resources, as such, it is important to understand the corresponding rates of burnout.
Similarly, infectious disease outbreaks have well-documented effects on the psychological wellbeing of healthcare workers (HCWs). During the Severe Acute Respiratory Syndrome (SARS), H1N1 and Ebola outbreaks, studies showed that frontline HCWs were at higher risk of developing psychological sequelae, including chronic stress, anxiety, depression and post-traumatic stress disorder [12–17]. Various factors are understood to have contributed to this phenomenon, such as excessive workload, concerns about occupational exposure, or infection of HCWs’ families. In comparison to previous pandemics, the psychological impact of Covid-19 may be more significant and widespread, given the scale of the pandemic [18–20].
This study aims to describe the prevalence and predictors of burnout, anxiety and depression in healthcare workers during the Covid-19 pandemic.
Institutional ethical approval was obtained for data collection in the United Kingdom and Poland by the Imperial College Research Ethics Committee (ICREC) Ref:20IC5890, and Singapore by the National Healthcare Group Domain Specific Research Board (NHS DSRB) Ref 2020–00598.
Countries selected for inclusion represented a range of Covid-19 mortality rates, health system design, economic development, and had regional coordinators that could adapt the questionnaire to the local context and champion distribution. See Table 1 for comparison of country settings.
| UK | Singapore | Poland | |
|---|---|---|---|
| Population (millions) | 66 | 5.7 | 38 |
| GDP ($) | 42,962 | 64,582 | 15,423 |
| Healthcare spend (% of GDP) | 9.6 | 4.4 | 6.5 |
| Per capita spend on healthcare ($) | 3,859 | 2,619 | 907 |
| Physicians/1,000 | 2.8 | 2.3 | 2.4 |
| Nurses & midwives/1,000 | 8.2 | 6.2 | 6.9 |
| Covid-19 cases* | 288,133 | 45,613 | 37,216 |
| Covid-19 deaths* | 44,650 | 26 | 1,562 |
| Healthcare funding | Public | Co-funding | Public |
| Healthcare provision | Public | Co-delivery | Public |
| National Lockdown/Circuit breaker | 23rd March 2020 | 7th April 2020 | 15th Mar 2020 |
| Initial government policies | Workplace closures School closures Public space closures Travel restrictions Reduction in elective services Temporary Nightingale hospitals | Workplace closures School closures Public space closures Travel restrictions Reduction in elective services Satellite clinics in temporary worker accommodation | Travel restriction School closures Reduction in public event capacity Designation of ‘infectious disease’ hospitals |
| Start government response stringency index± | 80 | 39 | 57 |
| End government response stringency index§ | 71 | 78 | 51 |
*As of 11th July 2020.
±Start of study period (27th Mar 2020).
§End of study period (16th June 2020).
The Government response stringency index is a composite measure, proposed by Hale et al, that integrates measures of ‘[Covid-19] containment and health’, ‘economic support’, and ‘[policy] stringency’ to form an overall index that can be used to compare government policy over time in different countries. The score represents the number and strictness of government policies and should not be interpreted as an ‘effectiveness score’[30].
The UK has 66 million residents [21]. Healthcare is publicly funded through general taxation and provided free at point of delivery by the National Health Service. The gross domestic product (GDP) is $42,962 per capita [22], of which 9.6% ($3,859) is spent on healthcare [23]. The UK has 2.8 physicians and 8.2 nurses and midwifes per 1,000 people [24,25]. The first documented case of Covid-19 was on 29th January 2020 and a national lockdown was initiated on 23rd March 2020 that introduced workplace, public space and school closures. In order to increase clinical capacity measures were taken including the cessation of elective services, redeployment of staff, reconfiguration of hospitals and establishment of a series of temporary ‘Nightingale’ hospitals. As of 11 July 2020 the UK has had 288,133 Covid-19 infections and 44,650 related deaths [26].
Singapore is a city-state of 5.7 million residents. 80% of hospital care is provided by the public sector [27] and is funded through a mixed-financing model of co-funding [28]. The GDP per capita is $64,582 [22], of which 4.4% ($2,619) is spent on healthcare [23]. Singapore has 2.3 physicians [24] and 6.2 nurses and midwives per 1,000 people [25]. Singapore reported its first case of Covid-19 on 23rd January 2020. In April, a national lockdown [29] was initiated that introduced workplace, public space, and school closures. In order to increase clinical capacity, non-urgent clinical procedures were reduced. As of 11 July 2020 Singapore has had 45,613 Covid-19 infections and 26 related deaths [26].
Poland has 38 million residents [21]. Healthcare is funded through the National Health Fund, general taxation and private insurance. The GDP per capita is $15,423 [22], of which, 6.5% ($907) is spent on healthcare [23]. Poland has 2.4 physicians and 6.9 nurses and midwives per 1,000 people [25,26]. On 4th March 2020, Poland reported its first case of Covid-19 and a national lockdown was initiated on 15th March 2020, which included border closures to foreign nationals and a quarantine for returning citizens. Twenty-three hospitals were repurposed into infectious diseases hospitals for patients with suspected or confirmed COVID-19 infection. A further 67 hospitals had an infectious disease ward available. As of 11 July 2020 Poland has had 37,216 Covid-19 infections and 1,562 related deaths [26].
The survey consisted of four parts; demographic questions followed by 3 validated psychometric instruments; the Safety Attitudes Questionnaire, Oldenburg Burnout Inventory and Hospital Anxiety and Depression Scale. Local collaborators in each country adapted the demographic questions to be culturally appropriate and contextually relevant. Demographic data included gender, ethnicity, professional role, workload, and Covid-19 status (see S1 File).
The OLBI is a 16-item validated tool for the investigation of burnout [31,32]. Items consist of both positively and negatively worded questions related to exhaustion and disengagement that are recorded on a four-point Likert scale. For the purpose of descriptive analyses, we considered participants to be at ‘high risk of burnout’ if they met the cut-offs of 2.1 and 2.25 for the exhaustion and disengagement subscales, respectively, as used in previous studies [33–36]. To increase specificity in the regression analyses, a higher cut-off of the 75th percentile of OLBI scores was used.
The HADS was developed in 1983 [37] and has since been widely used for assessing depression and anxiety [38]. It is self-reported, concise, and uses separate subscales for anxiety and depression, each consisting of seven items rated on a four-point Likert scale. It has been validated in several countries and adapted for use in different languages and settings [39–42]. A score of 7 or less is considered normal, 8–11 as borderline and greater than 11 is diagnostic of anxiety or depression. The HADS was used in studies evaluating the psychiatric morbidity amongst SARS survivors [43,44].
The Safety Attitudes Questionnaire (SAQ) measures staff perceptions of safety. It has been validated in several countries, languages [45–49] and healthcare settings, including critical care and inpatient wards [50]. Thirty-five statements were included, each followed by a 5-point Likert scale from “strongly disagree” to “strongly agree”. SAQ scores represent the proportion of respondents that “agree” or “strongly agree” with positive statements relating to each subscale, vice versa for negatively-worded questions [50] (S1 File). Scores are expressed across six domains: safety climate, teamwork, stress recognition, perception of management, working conditions, and job satisfaction. On all scales, a higher percentage score represents a more positive perception. Taken together, the scores provide insight into healthcare workers’ perceptions of operational conditions in their workplace.
Investigators in the UK and Singapore used English versions of the questionnaires. In Poland investigators utilised validated Polish versions of HADS, SAQ and OLBI. Demographic questions were translated by a native speaker (JP) and the translation validated through back translation by an independent native Polish speaker (GZ) (S1 File).
This cross-sectional study was conducted between 27th March and 16th June 2020. The questionnaire was administered using Google Forms (Google LLC, USA) in Europe, and FormSG (GovTech, Singapore) in Singapore. Invitations to participate were distributed using targeted email communications with weekly reminders, and advertisement on social media platforms (Twitter and Whatsapp). Written, informed consent was obtained from all participants. The study dataset was anonymized and uploaded (S2 File).
Allowing for up to 10 covariates in the multivariate model and a sensitivity of 0.05, a sample size of 2,000 participants was required.
Data were analysed using Stata v14 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station. TX: StataCorp LP). Reliability of each psychometric instrument (SAQ, OLBI, HADS) were assessed using Cronbach’s alpha. A complete case analysis approach was used. For each questionnaire, the values of each question were correlated with the individual’s total score. Alpha scores >0.70 were deemed as acceptable reliability. Statistical significance was set at 2-sided p < 0.05 using the Wald test The primary outcome measure was burnout, secondary outcome measures were anxiety and depression. Explanatory variables for burnout included SAQ scores, demographic questions, and HADS outcomes. Explanatory variables were assessed against the 75th percentile of OLBI scores using logistic regression. Variables found to be significant on univariate analysis were included in the multivariate analysis as well as forced variables that were deemed important to control for (country, role, and redeployment status). The “svy” command was used in the STATA setup for logistic regression.
A total of 3,537 responses were received (Table 2). Amongst these, 2,544 (72%) of respondents were female and 923 male (26.1%). 684 (19.3%) responses were from doctors, 1,590 (45%) from nurses, 517 (14.6%) from other clinical staff (including healthcare support workers, allied health professionals, pharmacists etc), and 746 (21.1%) non-clinical staff. 765 responses were from the UK, 232 from Poland, 2,503 from Singapore, and 37 from other countries, which were excluded due to the low response rate for the purpose of analysis to minimise a response bias. During the pandemic, 766 (21.7%) clinical staff were redeployed as part of response measures and 777 (22%) respondents had received at least one test for SARS-CoV-2 infection.

| Covariates | Overall (n = 3,537) | UK (n = 765) | Poland (n = 232) | Singapore (n = 2,503) | Pearson chi-square | |
|---|---|---|---|---|---|---|
| n | % | % | % | % | p-value | |
| Gender | <0.001 | |||||
| Male | 923 | 26.1 | 28.9 | 8.6 | 26.4 | |
| Female | 2544 | 71.9 | 69.9 | 90.5 | 71.3 | |
| Undisclosed | 70 | 2.0 | 1.2 | 0.9 | 2.4 | |
| Role | <0.001 | |||||
| Non-clinical | 746 | 21.1 | 14.1 | 1.7 | 25.3 | |
| Doctor | 684 | 19.3 | 35.7 | 8.2 | 14.5 | |
| Nurse | 1590 | 45.0 | 36.7 | 89.7 | 43.7 | |
| Other clinical staff | 517 | 14.6 | 13.5 | 0.4 | 16.5 | |
| Base Specialty | <0.001 | |||||
| Medicine | 1238 | 35.0 | 30.5 | 29.3 | 37.4 | |
| Surgery | 412 | 11.7 | 21.4 | 15.5 | 7.4 | |
| Acute | 388 | 11.0 | 16.9 | 16.8 | 8.7 | |
| Other specialty | 1055 | 29.8 | 26.7 | 38.4 | 30.2 | |
| Non-clinical | 433 | 12.2 | 4.6 | 0.0 | 15.9 | |
| Days Worked in Past Week | <0.001 | |||||
| 5 or less | 2651 | 75.0 | 76.0 | 84.9 | 74.0 | |
| 6 or more | 715 | 20.2 | 5.0 | 9.5 | 26.0 | |
| No response | 171 | 4.8 | 19.1 | 5.6 | 0.0 | |
| Redeployed | <0.001 | |||||
| No | 2771 | 78.3 | 62.8 | 89.7 | 82.1 | |
| Yes | 766 | 21.7 | 37.3 | 10.3 | 17.9 | |
| Redeployed Specialty | <0.001 | |||||
| Covid GM | 214 | 6.1 | 9.8 | 3.5 | 5.0 | |
| ITU/EM | 208 | 5.9 | 17.9 | 1.3 | 2.6 | |
| Other | 344 | 9.7 | 9.5 | 5.6 | 10.2 | |
| Treated Covid +ve patient in past week | <0.001 | |||||
| No | 1994 | 56.4 | 34.4 | 54.3 | 63.4 | |
| Yes | 853 | 24.1 | 54.1 | 17.7 | 15.3 | |
| Don’t know | 242 | 6.8 | 7.1 | 28.0 | 4.8 | |
| Not applicable | 448 | 12.7 | 4.4 | 0.0 | 16.5 | |
| Presence of Symptoms | <0.001 | |||||
| Asymptomatic | 3158 | 89.3 | 85.4 | 93.5 | 90.1 | |
| Symptomatic | 379 | 10.7 | 14.6 | 6.5 | 9.9 | |
| Testing Status | <0.001 | |||||
| Not tested | 2760 | 78.0 | 72.9 | 68.5 | 80.4 | |
| Tested | 777 | 22.0 | 27.1 | 31.5 | 19.6 | |
| Psychological Outcomes | n | % (95% CI) | % (95% CI) | % (95% CI) | % (95% CI) | |
| Burnout | 2364 | 67(65–68) | 63 (60–66) | 71(65–77) | 68 (66–70) | |
| Anxiety | 701 | 20(18–21) | 27 (24–30) | 28 (22–33) | 17 (15–18) | |
| Depression | 389 | 11(9–12) | 12 (9–14) | 14 (10–19) | 10 (9–12) | |
GM: General medicine; ITU: Intensive treatment unit; EM: Emergency medicine.
The questionnaires had strong reliability as evident by their high α coefficients (HADS α = 0.90, OLBI α = 0.88, SAQ α = 0.94). In our study, 2,364 (67%, 95% CI 65%-68%) of respondents were identified as being at high risk of burnout, whilst 701 (20%, 95% CI 18%-21%) and 389 (11%, 95% CI 9%-12%) met the criteria for anxiety and depression, respectively. A number of respondents met criteria for more than one condition (Fig 1).

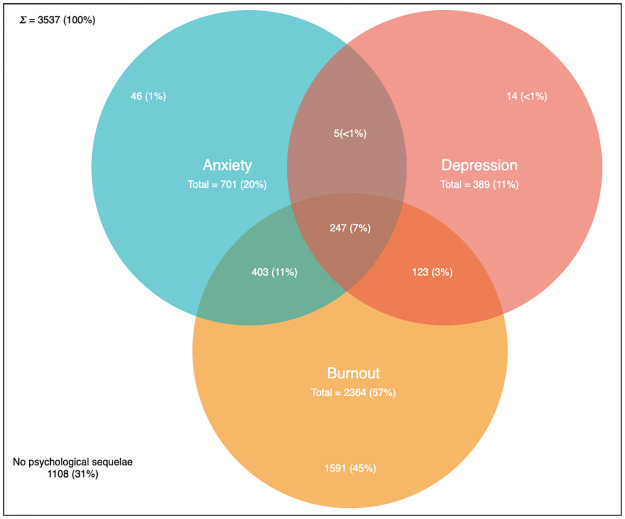
Venn diagram demonstrating prevalence of anxiety, depression and burnout in the sampled population.
This figure demonstrates the number of respondents meeting the OLBI criteria for burnout, the HADS criteria for anxiety and the HADS criteria for depression. The overlap of sets represent individuals meeting more than one criteria.
On univariate analysis (Table 3), significant covariates included undisclosed gender, job role, base specialty, redeployment, having been tested for Covid-19, treatment of patients with Covid-19, SAQ score, anxiety and depression. There was no significant relationship between, country, symptoms of Covid-19, number of days worked and burnout.
| Covariate | Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | p-value | 95% CI | OR | p-value | 95% CI | |||
| Base Specialty | ||||||||
| Medicine | Baseline | |||||||
| Surgery | 0.88 | 0.325 | 0.69 | 1.13 | ||||
| EM/ITU/Anaesthetics | 0.84 | 0.193 | 0.65 | 1.09 | ||||
| Other specialty | 0.81 | 0.021 | 0.67 | 0.97 | ||||
| Gender | ||||||||
| Male | Baseline | Baseline | ||||||
| Female | 1.15 | 0.107 | 0.97 | 1.37 | 0.94 | 0.618 | 0.75 | 1.19 |
| Undisclosed | 3.32 | <0.001 | 2.03 | 5.44 | 1.39 | 0.295 | 0.75 | 2.59 |
| Country | ||||||||
| UK | Baseline | Baseline | ||||||
| Poland | 1.36 | 0.058 | 0.99 | 1.86 | 1.30 | 0.196 | 0.87 | 1.95 |
| Singapore | 0.94 | 0.474 | 0.78 | 1.12 | 1.20 | 0.137 | 0.94 | 1.52 |
| Role | ||||||||
| Non-clinical | Baseline | Baseline | ||||||
| Doctor | 1.42 | 0.006 | 1.11 | 1.81 | 2.10 | <0.001 | 1.49 | 2.95 |
| Nurse | 1.54 | <0.001 | 1.25 | 1.90 | 1.38 | 0.026 | 1.04 | 1.84 |
| Other clinical staff | 1.64 | <0.001 | 1.27 | 2.13 | 2.02 | <0.001 | 1.45 | 2.82 |
| Days Worked in Past Week | ||||||||
| 5 or less | Baseline | |||||||
| 6 or more | 1.16 | 0.120 | 0.96 | 1.39 | ||||
| Redeployed | ||||||||
| No | Baseline | Baseline | ||||||
| Yes | 1.45 | <0.001 | 1.22 | 1.73 | 1.27 | 0.035 | 1.02 | 1.58 |
| Redeployed Specialty | ||||||||
| Not redeployed | Baseline | |||||||
| Covid GM | 1.28 | 0.113 | 0.94 | 1.74 | ||||
| ITU/EM | 1.59 | 0.002 | 1.18 | 2.14 | ||||
| Other | 1.49 | 0.001 | 1.17 | 1.89 | ||||
| Treated Covid +ve Patient in Past Week | ||||||||
| No | Baseline | |||||||
| Yes | 1.13 | 0.172 | 0.95 | 1.36 | ||||
| Don’t know | 2.09 | <0.001 | 1.59 | 2.75 | ||||
| Not applicable | 1.04 | 0.726 | 0.82 | 1.32 | ||||
| Presence of Symptoms | ||||||||
| Asymptomatic | Baseline | |||||||
| Symptomatic | 0.80 | 0.085 | 0.62 | 1.03 | ||||
| Testing Status | ||||||||
| Not tested | Baseline | Baseline | ||||||
| Tested | 0.80 | 0.016 | 0.66 | 0.96 | 0.64 | <0.001 | 0.51 | 0.82 |
| SAQ | ||||||||
| 50th Percentile | Baseline | Baseline | ||||||
| 25th Percentile | 3.48 | <0.001 | 2.92 | 4.15 | 2.43 | <0.001 | 1.98 | 2.99 |
| 75th Percentile | 0.29 | <0.001 | 0.22 | 0.38 | 0.30 | <0.001 | 0.22 | 0.40 |
| Anxiety | ||||||||
| Normal/Borderline | Baseline | Baseline | ||||||
| Abnormal | 8.23 | <0.001 | 6.86 | 9.87 | 4.87 | <0.001 | 3.92 | 6.06 |
| Depression | ||||||||
| Normal/Borderline | Baseline | Baseline | ||||||
| Abnormal | 10.06 | <0.001 | 7.92 | 12.78 | 4.06 | <0.001 | 3.04 | 5.42 |
OR: Odds ratio; EM: Emergency medicine; ITU: Intensive treatment unit; GM: General medicine.
On multivariate analysis (Table 3), the following predictors of burnout were: doctor role (OR 2.10; 95% CI 1.49–2.95), nursing role (OR 1.38; 95% CI 1.04–1.84), other clinical roles (OR 2.02; 95% CI 1.45–2.82), being redeployed (OR 1.27; 95% CI 1.02–1.58), SAQ score lower than the 25th percentile (OR 2.43; 95% CI 1.98–2.99), anxiety (OR 4.87; 95% CI 3.92–6.06) and depression (OR 4.06; 95% CI 3.04–5.42). Statistically significant factors that were inversely correlated with burnout included: being tested for Covid-19 (OR 0.64; 95% CI 0.51–0.82) and SAQ score higher than the 75th percentile (OR 0.30; 95% CI 0.22–0.40). SAQ score by psychological state is demonstrated in Fig 2.
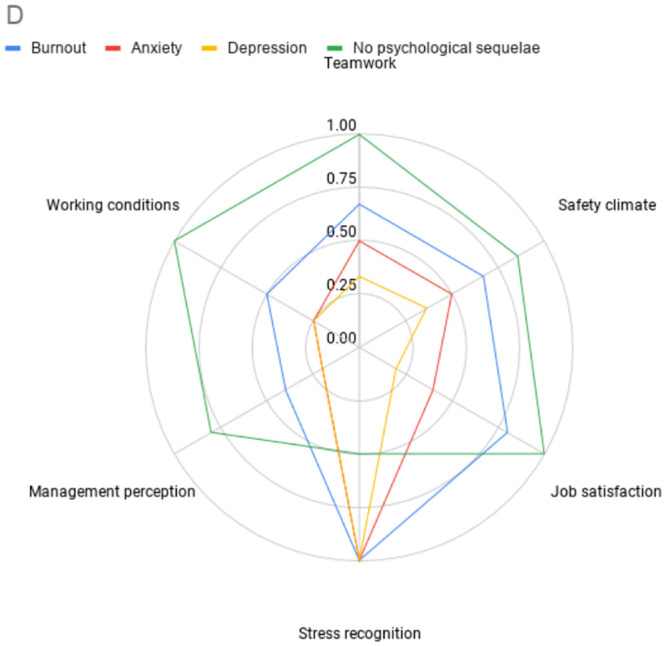
Radar plot demonstrating SAQ subscale by psychological state.
This figure demonstrates the SAQ subscale scores by psychological outcome. Distance from the centre represents proportion of a subscale answered positively. A greater distance represents a more positive score. § patients may be represented in more than one series. §§ Not all subscales are weighted equally in calculating overall SAQ score, the area of the radar plot will therefore not represent the overall SAQ score.
Significant predictors of depression (Table 4) included: being redeployed (OR 1.44; 95% CI 1.07–1.95), SAQ scores lower than the 25th percentile (OR 2.29; 95% CI 1.73–3.02), burnout (OR 4.18; 95% CI 3.13–5.57) and anxiety (OR 5.13; 95% CI 3.90–6.73). Significant factors inversely correlated with depression included: female gender (OR 0.62; 95% CI 0.45–0.84) and doctor role (OR 0.60; 95% CI 0.38–0.96).
| Covariate | Multivariate Analysis for Anxiety | Multivariate Analysis for Depression | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | p-value | 95% CI | OR | p-value | 95% CI | |||
| Gender | ||||||||
| Male | Baseline | Baseline | ||||||
| Female | 1.47 | 0.004 | 1.13 | 1.91 | 0.62 | 0.002 | 0.45 | 0.84 |
| Undisclosed | 2.12 | 0.025 | 1.10 | 4.08 | 0.76 | 0.462 | 0.36 | 1.58 |
| Country | ||||||||
| UK | Baseline | Baseline | ||||||
| Poland | 0.63 | 0.032 | 0.41 | 0.96 | 1.13 | 0.657 | 0.66 | 1.92 |
| Singapore | 0.48 | <0.001 | 0.37 | 0.61 | 1.07 | 0.675 | 0.78 | 1.48 |
| Role | ||||||||
| Non-clinical | Baseline | Baseline | ||||||
| Doctor | 1.13 | 0.511 | 0.78 | 1.63 | 0.60 | 0.031 | 0.38 | 0.96 |
| Nurse | 1.09 | 0.579 | 0.81 | 1.47 | 0.77 | 0.164 | 0.54 | 1.11 |
| Other clinical staff | 0.64 | 0.023 | 0.43 | 0.94 | 0.87 | 0.543 | 0.55 | 1.37 |
| Redeployed | ||||||||
| No | Baseline | Baseline | ||||||
| Yes | 1.14 | 0.297 | 0.89 | 1.45 | 1.44 | 0.015 | 1.07 | 1.93 |
| Testing Status | ||||||||
| Not tested | Baseline | Baseline | ||||||
| Tested | 1.28 | 0.055 | 1.00 | 1.64 | 1.18 | 0.29 | 0.87 | 1.61 |
| SAQ | ||||||||
| 50th Percentile | Baseline | Baseline | ||||||
| 25th Percentile | 2.19 | <0.001 | 1.74 | 2.76 | 2.29 | <0.001 | 1.73 | 3.02 |
| 75th Percentile | 0.88 | 0.41 | 0.66 | 1.19 | 0.74 | 0.185 | 0.48 | 1.15 |
| Burnout | ||||||||
| Low risk | Baseline | Baseline | ||||||
| High risk | 4.89 | <0.001 | 3.93 | 6.08 | 4.18 | <0.001 | 3.13 | 5.57 |
| Anxiety | ||||||||
| Normal/Borderline | Baseline | |||||||
| Abnormal | 5.13 | <0.001 | 3.90 | 6.73 | ||||
| Depression | ||||||||
| Normal/Borderline | Baseline | |||||||
| Abnormal | 5.15 | <0.001 | 3.91 | 6.78 | ||||
OR: Odds ratio.
Significant predictors of anxiety (Table 4) included: female gender (OR 1.47, 95% CI 1.13–1.91), undisclosed gender (OR 2.12; 95% CI 1.10–4.08), SAQ scores lower than the 25th percentile (OR 2.19; 95% CI 1.74–2.76), burnout (OR 4.89; 95% CI 3.93–6.08) and abnormal depression scores (OR 5.15; 95% CI 3.91–6.78). Factors inversely correlated with anxiety included: being from Poland (OR 0.63; 95% CI 0.41–0.96), being from Singapore (OR 0.48; 95% CI 0.37–0.61) and other clinical job role (OR 0.64; 95% CI 0.43–0.94).
In our study, 2,364 (67%) respondents were at high risk of burnout. Prior to the onset of Covid-19 studies reported rates of burnout in the UK of 31.5% [51] and 42% [52] for doctors and nurses, respectively. In Singapore figures were similar with 33% [53] and 51% [54] of nurses and doctors exhibiting symptoms of burnout, respectively. The higher rates observed in this study suggest that the Covid-19 pandemic, or changes as a result of the pandemic may have led to an increased rate of burnout amongst staff.
Our results demonstrate that clinical roles confer a higher burnout risk compared with non-clinical roles. This may be explained by the nature of these roles. Particular challenges might have included adapting to a new method of working, increased service demands, prolonged periods wearing personal protective equipment, feeling “powerless” to manage patients’ conditions, and a fear of becoming infected or infecting others [55]. Similar findings were seen in Toronto during the SARS epidemic, where HCWs that treated SARS patients had significantly higher levels of burnout than those that did not [6].
Staff who were redeployed to new clinical areas had a higher risk of burnout. This may be due to physical conditions such as spending prolonged periods wearing protective equipment or due to the stress of adapting to a new clinical environment. Moreover, areas that required redeployed staff, by definition, had (or anticipated having) demand in excess of resources, necessitating the reallocation of staff. The combination of these increased demands, limited resources, and the psychological stress of dealing with an unfamiliar disease in an unfamiliar environment may have led to increased rates of burnout. This hypothesis would be supported by by the demands-resources model of burnout [7,11].
Anxiety and depression were noted in 20% and 11% of respondents respectively. Respondents with anxiety or depression were likely to also have symptoms of burnout. This is a significant burden of psychological morbidity. This finding is consistent with a recent meta-analysis of studies in China and Singapore, which demonstrated that approximately 1 in 5 HCWs have experienced symptoms of anxiety (23.2%) or depression (22.8%) during Covid-19 [18]. Similarly, rates of depression (19.8%) were also seen in Italian HCWs, although with a lower prevalence of anxiety(8%) [19]. Our study found that anxiety was more prevalent than depression amongst HCWs. To our best knowledge, there has been no published work reporting rates of depression, anxiety or burnout in the UK or Poland during Covid-19.
Female gender was predictive of anxiety (OR 1.47), which is in keeping with previous findings during Covid-19 [56,57]. However female gender was also found to be inversely correlated with depression, which contrasts from previous research [56,57]. These findings may reflect differences in the sampled population, such as the proportion of redeployed staff or be related to the timing of sampling compared with the onset of the Covid-19 pandemic.
Burnout, anxiety and depression have a negative impact on staff and patient outcomes [9,58] as well as leading to workforce attrition [59]. The high rates seen during the Covid-19 pandemic risk compounding a pre-existing healthcare workforce crisis [60,61], which may inturn impact on patient outcomes during the recovery phase of the pandemic. Initiatives shown to have a positive effect on psychological wellbeing include: clear communication, access to personal protective equipment, adequate rest, and psychological support [57,62].
An unexpected finding was the inverse relationship between staff SARS-CoV-2 testing and mental health. Two possible explanations exist: 1. provision of testing is a proxy for a well-run organisation, staff feeling well supported feel positively about working conditions and perception of management and, in turn are less likely to develop adverse mental health outcomes. 2. Staff suffering from burnout, anxiety or depression were less likely to seek out testing, possibly due to disengagement, physical or psychological symptoms [63]. Irrespective of the cause, both explanations are important as they support the need for staff testing, in particular for staff groups identified at risk of Covid-19 or poor mental wellbeing.
Safety attitudes were significantly associated with psychological outcomes in this study. It cannot be determined whether safety attitude is a contributory factor for burnout, anxiety, and depression, or if these psychological states lead to poor safety attitudes. However, this is an important finding, as safety attitudes are both modifiable and independently associated with clinical outcomes [50,64,65]. The SAQ domains can be divided into net causes (teamwork, working conditions, safety climate subscales) and net effects (perception of management, job satisfaction, stress recognition) [66]. This suggests that in addition to supporting psychological wellbeing, initiatives that promote safety climate, working conditions, and teamwork may have benefits on safety attitudes and in turn psychological outcomes.
There are some limitations to our approach. The countries investigated are well stratified by: Covid-19 death rate, gross domestic product and geographic region (Western Europe, Eastern Europe and Asia-Pacific). However, the use of convenience sampling (a combination of social media and targeted email communications), means it is difficult to estimate response rate, response bias, and external validity. However, this study recruited a large number of respondents in a multi-centre, international population with a diverse range of healthcare workers. The results are therefore likely to be internally valid and associations between covariates reliable. Our sample was 72% female, which is broadly in line with the demographics of the healthcare workforce in the countries studied [67,68]. There was wide variation in the number of respondents between countries and an overrepresentation of nurses in the Polish cohort, this alongside data on only a limited number of variables may have resulted in residual confounding on multivariate regression analyses.
While the OLBI has many good psychometric qualities, a clinical cut-off for when someone is considered “burned out” has been an issue of debate [69]. The cut-off values used in this study to describe prevalence are based on findings from a Swedish group as correlated with clinician-diagnosed burnout [70,71]. The same cut-off values have been adopted in multiple other studies [34–36]. Given the high prevalence of burnout in this sample, and a lack of universally agreed cut-offs when using the OLBI, to improve specificity we used the 75th percentile of burnout scores rather than (lower) cut-offs values for the purpose of regression analyses.
While investigating the prevalence of psychological findings during Covid-19 is important, it is unclear if findings are as a direct result of Covid-19. It is also unclear if acute derangements persist over time. Repeated measurements will be needed to identify any potential long-term effects of the Covid-19 pandemic.
Finally, the contextual differences between participating countries, may limit the extent to which direct comparisons can be drawn between study countries.
Based on these findings, we outline several preliminary recommendations that may positively impact on the psychological health of HCWs and patient safety.
As highlighted by the association between safety attitudes and psychological outcomes, institutions should pay particular attention to safety culture during the Covid-19 pandemic. The use of patient safety teams, for example, can support the integration of human factors principles, such as effective communication, into organizational processes that will improve patient and staff safety [72]. The use of such teams during a time of organisational change can help “design, adapt and reconfigure work systems, maximize individual and team performance under high-risk, high-stakes environments, while minimizing the introduction of new significant safety risks or unintended consequences into the work system”. Similarly, institutions should boost and expand learning systems to capture risks and improvement opportunities, and leverage these to protect staff and patients. This is of particular importance given the limited evidence about the effects of Covid-19 on patients, staff and institutions [73].
Previous research has suggested that burnout is a precursor to depression [74], consequently, benefit may been seen from interventions to address burnout before the onset of depression or anxiety. At the individual level, evidence-based interventions include mindfulness, self-awareness exercises, and appreciative interviews [75]. At the organizational level, quality improvement projects that improve organizational communication and streamline workflows can reduce burnout rates [76].
Measures to mitigate harm arising from psychological distress following the Covid-19 pandemic are important to prevent long-term harm. Greenburg et al [77] proposed six evidence-based principles to support the mental health of HCWs following the Covid-19 pandemic: appropriate appreciation, investigating absences (for welfare reasons), conducting return to work interview, paying close attention to at-risk groups, continually monitoring staff, and helping HCWs make sense of their experience.
Further research is needed to investigate the mechanisms underlying the associations identified in this study. Interrupted time series or longitudinal studies would be appropriate to investigate chronicity of findings and generate hypotheses about causality. Alongside this, interventions to reduce psychological harm or improve safety culture should be evaluated for efficacy, with case control or ideally, randomized-controlled designs.
Our findings demonstrate a significant burden of burnout, anxiety, and depression amongst healthcare workers. A strong association was seen between SARS-CoV-2 testing, safety attitudes, gender, job role, redeployment and psychological state. These findings highlight the importance of targeted support services and proactive SARS-CoV-2 testing of healthcare workers.
We would like to thank the Pansurg collaborative for support and infrastructure supporting this project. We would like to thank Patient Safety Watch for support and advice relating to safety attitudes and patient safety in this paper.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
 Determinants of burnout and other aspects of psychological well-being in healthcare workers during the Covid-19 pandemic: A multinational cross-sectional study
Determinants of burnout and other aspects of psychological well-being in healthcare workers during the Covid-19 pandemic: A multinational cross-sectional study
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
